B39M, en-route, Beaverton OR USA, 2024
B39M, en-route, Beaverton OR USA, 2024
Summary
On 5 January 2024, a Boeing 737-9 which had just departed Portland was climbing through 14,800 feet when there was a loud bang followed by a rapid decompression. This resulted from the loss of a fuselage plug incorrectly installed at an unused door location during completion of the airframe manufacturing process. An emergency was declared and a landing back at Portland was made after a total of twenty minutes airborne. The investigation found that the fuselage plug involved was installed without being properly secured and identified deficiencies in the manufacturer's quality assurance processes as well as in the regulatory oversight.
Flight Details
Aircraft
Operator
Type of Flight
Public Transport (Passenger)
Flight Origin
Intended Destination
Actual Destination
Take-off Commenced
Yes
Flight Airborne
Yes
Flight Completed
Yes
Phase of Flight
Climb
Location
General
Tag(s)
Air Turnback,
Inadequate Airworthiness Procedures,
Ineffective Regulatory Oversight,
CVR overwritten
LOC
Tag(s)
Airframe Structural Failure
EPR
Tag(s)
“Emergency” declaration
CS
Tag(s)
Pax oxygen mask drop
AW
System(s)
Airframe
Contributor(s)
Maintenance Error (valid guidance available),
Component Fault after installation,
In flight separation of failed component
Outcome
Damage or injury
Yes
Aircraft damage
Major
Non-aircraft damage
No
Non-occupant Casualties
No
Occupant Injuries
Few occupants
Occupant Fatalities
None
Off Airport Landing
No
Ditching
No
Causal Factor Group(s)
Group(s)
Aircraft Technical
Safety Recommendation(s)
Group(s)
Aircraft Operation
Aircraft Airworthiness
Investigation Type
Type
Independent
Description
On 5 January 2024, a Boeing 737-9 (N704AL) which had only recently been delivered to Alaska Airlines was used on a scheduled domestic passenger flight from Portland to Ontario CA as AS1282. It was climbing through 14,800 feet in day visual conditions (VMC) six minutes after takeoff when a loud bang was followed by a rapid decompression. The immediate cause was the appearance of a door-sized opening in the rear cabin. The crew declared an emergency and the flight landed back at Portland fourteen minutes later. No passengers were immediately adjacent to the opening, and the injuries to seven passengers and one of the cabin crew in the vicinity were minor. Minor internal damage occurred to the passenger cabin in the immediate vicinity of the opening. The piece of detached fuselage structure was found in the back yard of a private house in Beaverton and recovered for examination, but most of the associated bolts and fittings were not found.

A view from the aircraft interior showing a hole in the left fuselage at row 26. [Reproduced from the Official Report]
Investigation
An accident investigation is being carried out by the U.S. National Transportation Safety Board (NTSB). Relevant data was downloaded from the flight data recorder (FDR) but data from the two-hour cockpit voice recorder (CVR) was overwritten because it was not isolated in time after the flight landed. Recorded ATC communications during the flight were available.
The 48-year-old captain had a total of approximately 12,700 hours flying experience, which included approximately 6,500 hours on type. Since the operator had begun taking delivery of the aircraft type variant, he had flown 304 hours on it. The 36-year-old first officer had a total of approximately 8,300 hours flying experience, which included approximately 1,500 hours on type. Since the operator had begun taking delivery of the aircraft type variant, she had flown 311 hours on it.
What Happened
The flight took place with the captain as pilot flying (PF), and after departure from runway 28L was cleared to climb to FL 230. Following the loud bang, when the fuselage panel was lost and decompression occurred, both pilots reported that their ears popped. The aircraft was climbing through 14,800 feet and reached a maximum altitude of 16,320 feet before the captain initiated a descent. He reported that when the noise and decompression occurred, he was pushed forward and his headset was dislodged so that it nearly fell off his head. The first officer said her headset was completely removed by the rapid outflow of air from the flight deck. Both pilots reported that they immediately donned their oxygen masks. They also said the flight deck door had been blown open and that it was very noisy and difficult to communicate with each other. They contacted air traffic control (ATC), declared an emergency and requested a lower altitude. Clearance to 10,000 feet was given and the crew completed the rapid decompression checklist. Further descent and positioning for a runway 28L approach proceeded without further event. Landing was followed by taxi to the gate for a normal disembarkation. It was found that following decompression, all cabin crew and passenger oxygen masks had deployed immediately as required. The flight crew reported that the locked flight deck door had opened during the depressurisation. It was noted that in a flight crew operating manual (FCOM) revision issued eight days after the accident, Boeing confirmed that this was in accordance with the design of the door.
Damage to the aircraft structure was assessed by the investigation to have been “substantial” on the basis that it had affected the structural strength of the aircraft. Damage in the passenger cabin was found to have included damage to seat rows 25ABC and 26ABC (seat 25A was rotated out and rearwards by approximately 10°- 20° towards the opening and the back of seat 26A was rotated forward and outboard towards the opening) as well as deformation of the forward toilet doorframe and “buckling and displacement of the sidewall panels and trim” from rows one through 27.
Why It Happened
It was immediately recognised that the missing fuselage plug was one of two which had been fitted in place of optional “Mid Exit Doors” (MEDs) on each side of the aircraft behind the wing (see the illustration below). These MEDs are required to meet emergency exit requirements when the longest 737 variants are configured with the maximum possible number of seats which was not the case with Alaska Airlines’ fleet.
It was noted that the airline had, like some other operators, decided not to configure its aircraft to the maximum possible passenger capacity for a number of reasons. These included the reduced weight of (28.5kg for the MED plug instead of 68kg for a door), the provision of a full-sized passenger window in the MED and because a plug lacks the complexity of a door, which has more parts and associated maintenance concerns.
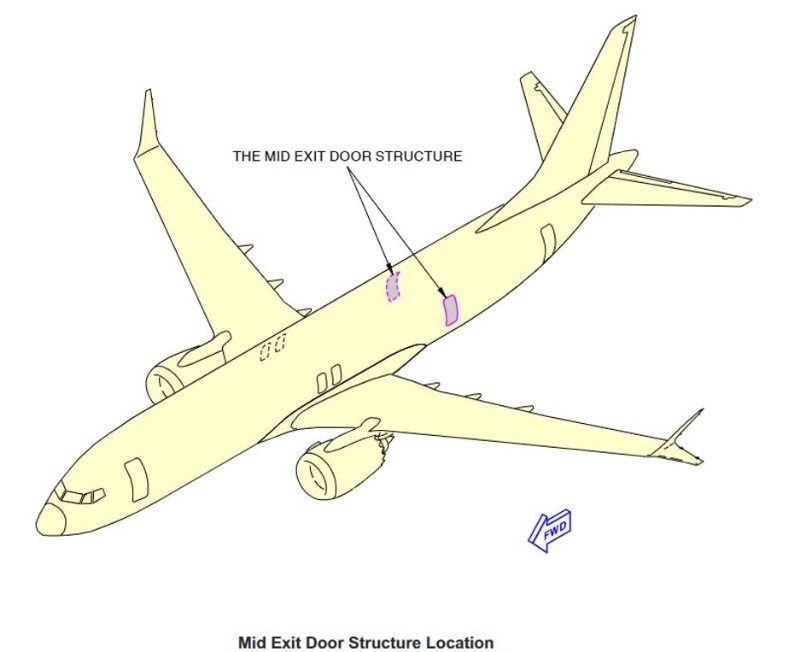
The location of the MEDs. [Reproduced from the Official Report]
It was established that the accident MED plug was manufactured by Spirit AeroSystems in Malaysia on 24 March 2023 and received by Boeing subcontractor Spirit AeroSystems in Wichita on 10 May 2023. It was then installed on the fuselage by Spirit before being shipped to Boeing by rail on 20 August 2023 and arriving at Boeing’s facility at Renton eleven days later.
It was noted that the MED plug is installed in the fuselage by means of two upper guide fittings and two lower hinge fittings. The two upper guide fittings engage with two upper guide rollers which are fixed to the upper sides of the opening. The two lower hinge guide fittings engage with two lower hinge fittings which are attached to the lower hinge bracket assemblies at the bottom of the plug. Once the plug is in place, it is secured from moving vertically by four bolts, one at each upper guide fitting and one at each lower hinge guide fitting. These four bolts are secured using castellated nuts and cotter pins. Any outboard motion of the plug is prevented by 12 stop fittings (six along each forward and aft edge) which are installed on the fuselage door frame structure. The door plug is only intended to be partially opened (by means of the hinge at its base) for maintenance and inspection which is only possible once the four previously mentioned bolts have been removed.
The report stated: "The [NTSB] found that the four bolts that secured the left MED plug to prevent it from moving upward vertically were missing before the newly manufactured airplane was delivered to Alaska Airlines. As a result, the left MED plug was able to become displaced gradually upward (by fractions of an inch) during previous flights until, during the accident flight, it displaced upward enough to disengage from its stop fittings and separate in flight."
Separately, it was established that once the fuselage arrived at the Boeing facility at Renton, it was found that a Boeing Non-Conformance Record had been raised noting five damaged rivets on the edge frame forward of the subject MED plug. In order to replace the damaged rivets, it was necessary to open the MED plug which required removal of the four bolts securing the two upper guide fittings and the two lower hinge guide fittings. This replacement was carried out on 19 September 2023 but a photo taken later the same day after the MED plug had been closed showed that the three retention bolts which should have been visible (one is obscured by insulation, the other three locations are circled on the illustration below) had not been fitted.
.

The MED Plug after rivet rectification work. [Reproduced from the Official Report]
The investigation was satisfied that the MED plug was not opened after the rivet rectification work completed on 19 September. This meant that all four bolts which prevent an installed MED plug from moving vertically upwards were either removed and not replaced at Renton during the work on 19 September or were not fitted when the fuselage arrived from Wichita. Thereafter, the Investigation focused on Boeing’s safety management system (SMS) and Spirit AeroSystems’ ongoing development of its own voluntary SMS program and at the U.S. Federal Aviation Administration's (FAA) involvement in the development of both these SMS programs and the level and effectiveness of FAA regulatory oversight applied in each case.
Safety Action as a result of the initial findings of the Investigation was noted to have included the following:
- The immediate grounding by the operator of its fleet of B737-9 aircraft so that inspection of all MED plugs could begin the following day.
- The issue by the FAA the day following the accident of an emergency airworthiness directive (AD) requiring all operators of the aircraft type variant to conduct specific related inspections before returning them to service.
- The issue by FAA on 21 January 2023, a SAFO (Safety Alert for Operators) recommending all operators of Boeing 737-900ER with a different variant of the same MED plug as the accident aircraft to inspect the four locations where the retaining hardware secures the MED plug to the airframe as soon as possible.
- The issue by Boeing on 24 January of a Multi-Operator Message (MOM) containing revised instructions for inspecting 737-9 aircraft that have the MED plugs.
The rest of the Investigation was focused on establishing whether the maintenance error which had occurred was indicative of wider systemic risk in airframe assembly standards or an isolated case within a generally safe system. A comprehensive review determined that the plug door loss indicated that working practices associated with airframe manufacture at Boeing - and specifically the quality control oversight of work by contractors - was inadequate. Extensive assessment eventually disclosed that the extent of this problem was potentially much wider than just contactors. Two specific and important safety issues were identified, documented and analysed in the Final Report:
- Quality assurance processes and oversight deficiencies, including Boeing’s ineffective change management related to workforce experience level decreases and Boeing’s ineffective corrective actions and the FAA’s ineffective oversight processes that allowed the persistence of issues with Boeing’s Business Process Instruction for parts removals.
- The need for Boeing to improve its quality escape mitigation strategies and continue its development and implementation of its SMS.
Other less individually complex secondary safety issues than the two above were also identified including:
- The need for flight crew hands-on emergency oxygen mask training.
- The need to ensure that the design standards for portable oxygen bottles ensure that the associated masks are easier to unpack and use.
- The need for effective aircraft operator procedures and 25-hour CVR installations and retrofits to prevent the loss of CVR audio after accidents and serious incidents.
- The safety benefits of using Child Restraint Systems (CRS) for children under the age of 2 years.
The Key Findings of the Investigation were, in summary, as follows:
- There was no evidence that Alaska Airlines performed any maintenance, inspection, or retrofit work on the airplane that would have involved opening the left mid-exit door plug.
- The left mid exit door (MED) plug had displaced incrementally upward during previous flights before it displaced upward to the extent where the stop pin to stop pad contact became unstable allowing it to move upward, outboard and aft as it separated from the fuselage.
- Prior to its loss overboard, the upward migration of the left MED plug prior to the accident flight would not have been readily detectable by a pilot performing a routine pre-flight external inspection.
- The aircraft cabin pressurisation system operated as designed both before and after the left MED plug separated and there was no evidence that previous pressurisation auto fail light illumination events on the same aircraft had been associated with upward displacement of the MED plug during previous flights.
- The flight crew responses to the consequent rapid depressurisation and use of the “Cabin Altitude or Rapid Depressurisation” Checklist were consistent with company procedures, their decision to descend the airplane and return to the departure airport was a timely and appropriate emergency response. They demonstrated effective high-workload management and task allocation appropriate for a two-person crew to safely handle the emergency.
- The absence of bolt contact damage or deformation around the holes associated with the vertical movement arrestor bolts and upper guide track bolts indicates that the four bolts that should have been installed to prevent the left mid exit door plug’s upward movement were missing before the plug moved upward off the stop pads.
- The left mid exit door plug’s vertical movement arrestor bolts, upper guide track bolts, and associated hardware were installed before the fuselage was delivered to Boeing but subsequently removed during the manufacturing process when the plug was opened to facilitate additional work. None of the personnel involved had any experience with opening a MED plug and none said they knew who had opened it.
- Whoever did open the left mid exit door plug failed to document this action which increased the risk that the closure would not be performed properly and validated by a quality assurance inspection.
- Boeing Commercial Airplanes’ Business Process Instruction “Perform Part or Assembly Removal” lacked clarity, conciseness, and ease of use necessary to be effective.
- Boeing Commercial Airplanes’ on-the-job training was unstructured, undocumented, and focused primarily on routine build tasks, which meant that it was less likely personnel with limited exposure to non-routine tasks would be able to correctly perform the task of opening a mid exit door plug.
- Only door team personnel were allowed to perform work on doors and mid exit door (MED) plugs, but none were on duty at the time the left MED plug was closed.
- The post-accident design enhancement of the mid exit door (MED) plug, if certified by the Federal Aviation Administration and implemented by Boeing Commercial Airplanes, will help ensure the complete closure of an MED plug following opening or removal.
- Because Boeing Commercial Airplanes’ did not conduct a change management assessment to identify and address the risks associated with using a workforce with reduced experience, including hiring many with little or no previous manufacturing experience, it missed an opportunity to proactively implement mitigations to ensure quality standards were maintained.
- Despite being accepted by the Federal Aviation Administration, Boeing Commercial Airplanes’ corrective actions to address persistent deficiencies with their Business Process Instruction “Perform Part or Assembly Removal”, such work had a documented history of compliance issues for at least 10 years before the accident.
- The Federal Aviation Administration’s compliance and enforcement surveillance, audit planning assessments, and records systems of Boeing Commercial Airplanes were deficient and lacked the functionality necessary to identify repetitive and systemic discrepancies and non-conformance issues with their Business Process Instruction “Perform Part or Assembly Removal”, including previous instances of undocumented part removals.
- Boeing Commercial Airplanes’ quality escape guidance, which focused on components rather than the actions of people performing tasks, did not adequately address controls for human error so that their ability to identify and build effective mitigation strategies was compromised.
- In the 2 years before the accident airplane’s production, Boeing Commercial Airplanes’ voluntary safety management system was an immature program that lacked formal Federal Aviation Administration oversight and did not proactively identify the risk of the quality escape that occurred.
- Having a fully developed SMS implemented at every level of the quality management and production process, would provide Boeing Commercial Airplanes with a systematic approach to proactively identifying and managing the human risks associated with aircraft production.
- For future implementation of Boeing Commercial Airplanes’ regulatory safety management system and integration into its quality management system to be successful, accurate and ongoing data about its safety culture is needed.
- While hands-on oxygen mask simulator training was provided to the flight crew before the accident, it lacked realistic scenario-based exercises and, therefore, failed to adequately prepare them for potential real-world events.
- Although the portable oxygen bottles used by the flight attendants met Federal Aviation Administration design standards, the difficulties the flight attendants encountered when using the masks, including the need to improvise a tool to open the packaging, suggest that the standards, the mask design, or both do not adequately consider ease of use and quick donning in an emergency.
- Alaska Airlines’ procedures at the time of the accident were ineffective in ensuring that data were preserved from the accident flight, resulting in the loss of critical information for the investigation. The circumstances of this and other accidents show 25-hour CVRs are necessary.
- The Federal Aviation Administration’s emphasis on increasing voluntary usage of child restraint systems, rather than mandating their use has continued to allow children under the age of 2 years to travel on board aircraft at a lower level of safety than that of seat belt-wearing adult passengers. Although none of the three lap-held children on board the airplane sustained injury, the circumstances of this accident and others show that the potential for severe injury or death exists for children less than 2 years old who are not secured in a child restraint system appropriate to their size and weight.
The Probable Cause of the Accident was determined to have been “the in-flight separation of the left mid exit door (MED) plug due to Boeing Commercial Airplanes’ failure to provide adequate training, guidance and oversight necessary to ensure that manufacturing personnel could consistently and correctly comply with its parts removal process, which was intended to document and ensure that the securing bolts and hardware that were removed from the left MED plug to facilitate rework during the manufacturing process were reinstalled”.
A Contributing Factor to the Accident was assessed to have been “the Federal Aviation Administration’s ineffective compliance enforcement surveillance and audit planning activities, which failed to adequately identify and ensure that Boeing addressed the repetitive and systemic non-conformance issues associated with its parts removal process".
A total of 19 New Safety Recommendations were made as follows:
- that the Federal Aviation Administration (FAA), once the certification of Boeing Commercial Airplanes’ design enhancement for ensuring the complete closure of Boeing 737 Mid Exit Door (MED) plugs following opening or removal, issue an Airworthiness Directive to require that all in-service MED plug-equipped airplanes be retrofitted with this design enhancement. [A-25-15]
- that the Federal Aviation Administration (FAA) revise the compliance enforcement surveillance system to ensure that it provides the necessary functionality for Federal Aviation Administration managers and inspectors overseeing production approval holders to effectively identify, record, track, and resolve recurring and systemic discrepancies and non-conformance issues, including those related to specific manufacturing processes. [A-25-16]
- that the Federal Aviation Administration (FAA) revise audit planning activities to ensure that they provide the necessary functionality for Federal Aviation Administration managers and inspectors overseeing production approval holders to effectively identify, record, track, and resolve recurring and systemic discrepancies and non-conformance issues, including those related to specific manufacturing processes. [A-25-17)
- that the Federal Aviation Administration (FAA) revise records systems to ensure that they provide the necessary records for Federal Aviation Administration managers and inspectors overseeing production approval holders to effectively identify, record, track, and resolve recurring and systemic discrepancies and non-conformance issues, including those related to specific manufacturing processes. [A-25-18]
- that the Federal Aviation Administration (FAA), once the actions in Safety Recommendations A-25-16, A-25-17 and A-25-18 are completed, develop guidance for Federal Aviation Administration managers and inspectors who provide oversight of production approval holders on how to identify, record, track, and effectively address repetitive and systemic discrepancies and non-conformance issues, to include strategies for assessing the effectiveness of corrective actions taken by the production approval holder during the previous year when developing next year’s certificate management plan. [A-25-19]
- that the Federal Aviation Administration (FAA), once the actions in Safety Recommendation A-25-19 are completed, provide Federal Aviation Administration managers and inspectors who provide oversight of production approval holders with recurrent training on how to identify, record, track, and effectively address repetitive and systemic discrepancies and non-conformance issues, to include strategies for assessing the effectiveness of corrective actions taken by the production approval holder during the previous year when developing the next year’s certificate management plan. [A-25-20]
- that the Federal Aviation Administration (FAA) retain historical compliance enforcement surveillance and audit records older than 5 years and provide Federal Aviation Administration managers and inspectors access to these records to enhance their oversight planning for production approval holders. [A-25-21]
- that the Federal Aviation Administration (FAA) convene an independent panel to conduct a comprehensive review of Boeing Commercial Airplanes’ safety culture. The findings should be used to enhance the ongoing development of Boeing’s regulatory safety management system (SMS) and the integration of its SMS into its broader quality management system. [A-25-22]
- that the Federal Aviation Administration (FAA) notify operators of the circumstances of the Accident involving Alaska Airlines flight 1282 and encourage them to review their flight crew training programs and ensure that they include hands-on, aircraft-specific training and procedures for each type of oxygen system in the operators’ fleet (which) include establishing and maintaining communications when the oxygen masks are donned and removed while participating in realistic emergency procedures training scenarios. [A-25-23]
- that the Federal Aviation Administration (FAA) review and revise, as necessary, the design standards that apply to portable oxygen bottle design to ensure that they adequately address ease of use and quick donning in an emergency situation, including considerations for the effort needed to remove the mask from its packaging. [A-25-24]
- that the Federal Aviation Administration (FAA) require operators of airplanes equipped with a cockpit voice recorder (CVR) to incorporate guidance into company standard operating procedures, emergency protocols, and post-incident and post-accident checklists - as applicable to both flight crew and non-flight crew personnel - detailing actions to preserve CVR recordings as soon as practical after completion of a flight with a reportable event. [A-25-25]
- that the Boeing Company continue the certification process for the design enhancement for mid exit door plugs to ensure that, once the design enhancement is certified, all applicable newly manufactured airplanes are equipped with the enhancement. [A-25-26]
- that the Boeing Company, once the design enhancement for mid exit door (MED) plugs is certified, issue a service bulletin to address retrofitting in-service MED plug-equipped airplanes with the design enhancement. [A-25-27]
- that the Boeing Company should apply the updated safety risk management process to current and future revisions to Business Process Instruction “Perform Part or Assembly Removal” to ensure that it provides clear and concise guidance for determining when a removal record is needed. [A-25-28]
- that the Boeing Company develop recurrent training on Business Process Instruction “Perform Part or Assembly Removal” for Boeing manufacturing personnel that emphasises the importance of removal records for product safety, prepares personnel to consistently and correctly determine when a removal record is needed, and ensures that a removal record is generated when required. [A-25-29]
- that the Boeing Company develop a structured on-the-job training program that identifies and defines tasks necessary for manufacturing personnel to be considered fully qualified in their (jobs) and includes a grading system for trainers and trainees to track progress and determine competence. [A-25-30]
- that the Boeing Company document and archive the results of training provided and received as part of the program recommended in Safety Recommendation A-25-30 to support future data analysis. [A-25-31]
- that the Boeing Company revise the safety risk management process to ensure that it:
- identifies the root causes of manufacturing process compliance issues, like the persistent deficiencies with Business Process Instruction “Perform Part or Assembly Removal” and other production process inconsistencies identified in this investigation;
- evaluates the effectiveness of corrective actions. [A-25-32]
- that the Boeing Company, as the quality management system and safety management system are integrated, develop a process that can identify escapes that result from human error, assess them using a system specifically designed to identify factors that contribute to such errors, and implement effective mitigation strategies. [A-25-33]
In addition, 5 Previously Issued NTSB Safety Recommendations were formally reiterated as follows:
- that Federal Aviation Administration (FAA) require all newly manufactured airplanes that must have a cockpit voice recorder (CVR) be fitted with a CVR capable of recording the last 25 hours of audio. [A-18-30]
- that Federal Aviation Administration (FAA) require retrofit of all cockpit voice recorders (CVR) on all airplanes required to carry both a CVR and a flight data recorder with a CVR capable of recording the last 25 hours of audio. [A-24-9]
- that Federal Aviation Administration (FAA) conduct a study to determine the factors that affect caregivers’ decisions about the use of child restraint systems (CRSs) when travelling on a Title 14 Code of Federal Regulations Part 121 air carrier airplane with children under the age of 2 and to understand the challenges associated with using CRSs; publish the study findings. [A-21-40]
- that Federal Aviation Administration (FAA) after the action in Safety Recommendation A-21-40 is completed, use the study findings to direct the Administration’s efforts to increase child restraint system usage. [A-21-41]
- that Airlines for America, the National Air Carrier Association and the National Airline Association co-ordinate with (their) member airlines to develop and implement a program to increase child restraint system (CRS) usage in airplanes; this effort should include collecting data to determine the programme’s effectiveness at increasing CRS usage. [A-21-45]
The 158-page Final Report of the Investigation was completed on 24 June 2025.