B738, en-route, north Lincolnshire UK, 2023
B738, en-route, north Lincolnshire UK, 2023
Summary
On 17 October 2023 a Boeing 737-800 passing FL130 after departing Manchester received a cabin pressurisation warning, and the crew recognised that both engine air bleeds were off. After correcting this, climb was continued without donning oxygen masks until an air conditioning pack fault occurred, which prompted the operator to request a return which was uneventful. The bleeds-off condition had arisen after maintenance and had then not been recognised at release to service or during crew preflight checks.
Flight Details
Aircraft
Operator
Type of Flight
Public Transport (Passenger)
Flight Origin
Intended Destination
Actual Destination
Take-off Commenced
Yes
Flight Airborne
Yes
Flight Completed
Yes
Phase of Flight
Climb
General
Tag(s)
Air Turnback,
CVR overwritten
HF
Tag(s)
Inappropriate crew response (technical fault),
Plan Continuation Bias,
Procedural non compliance,
Violation
LOC
Tag(s)
Significant Systems or Systems Control Failure,
Flight Management Error
AW
System(s)
Air Conditioning and Pressurisation,
Bleed Air
Contributor(s)
Maintenance Error (valid guidance available)
Outcome
Damage or injury
No
Non-aircraft damage
No
Non-occupant Casualties
No
Off Airport Landing
No
Ditching
No
Causal Factor Group(s)
Group(s)
Aircraft Operation
Aircraft Technical
Safety Recommendation(s)
Group(s)
None Made
Investigation Type
Type
Independent
Description
On 17 October 2023 a Boeing 737-800 (G-TAWD) operated by TUI Airways on an international passenger flight from Manchester to Kos Airport, Greece, was in the climb at FL130 in unspecified day flying conditions when a cabin altitude warning was activated. Pressurisation was initiated by selecting the engine bleeds on but the corresponding checklist was not actioned. The cabin remained above 10,000 feet for over 40 minutes without flight crew use of supplemental oxygen until an air conditioning pack fault after further climb then led to an air turnback on request from the aircraft operator.
Investigation
An investigation was carried out by the UK Air Accident Investigation Branch (AAIB). Relevant recorded data were recovered from the flight data recorder (FDR), but corresponding data on the cockpit voice recorder (CVR) had been overwritten. Supporting information was also available from the quick-access recorder (QAR).
The 53-year-old captain, who was acting as pilot flying (PF) for the sector had a total of 18,000 hours flying experience which, included 1,600 hours on type. No age or experience information was given for the first officer. Both pilots had been rostered on Standby from 0400L but were advised shortly before commencement of this duty period that they were required to report at 0530L to operate a flight to Kos. The captain reported for the flight on time but received a call from the first officer to say that they had been delayed by an unexpected road closure so it was agreed that the captain would take over all predeparture preparations including external and internal checks. The first officer arrived at the aircraft at 0700L as the passengers were boarding, having reported that they had downloaded the operational flight plan (OFP) and reviewed the weather and aircraft status before leaving home. The pilots had flown together on previous flights and both recalled that they had not felt under pressure. The captain had said that whilst an on-time departure was desirable, preparing the aircraft correctly was of more importance.
What Happened
The flap 5 departure was uneventful and the autopilot (AP) was engaged once the After Takeoff checks had been completed. These included a check that both bleed air switches were selected on so that the aircraft would pressurise during the climb as cleared to FL280. However, passing FL130, FDR data showed that the cabin altitude had reached 10,000 feet and the aural cabin altitude warning horn had been activated. A request to Air Traffic Control (ATC) to level off at FL150 was made and approved and, according to the captain’s subsequent report, “it was quickly noticed that both engine bleeds were off, these were placed straight back on and the problem was resolved." FDR data showed that in fact the two engine bleeds had not been switched on for over a minute, during which the aircraft had been levelled at FL150. Once at that level, it was stated that “the (relevant non-normal checklist (NNC) in the) QRH had been actioned". However the investigation established that in reality, “neither pilot actioned the QRH Cabin Altitude Checklist” (see below) and its memory items, including the immediate use of oxygen masks, were not complied with. The captain stated that he had considered that “as the bleed systems were now on and.....the situation under control, he had decided that the memory items, including the use of oxygen masks, were disproportionate to the situation." Having further recalled seeing that the indicated cabin altitude had reached 2,000 feet “within a couple of minutes of the engine bleed switches being selected on," he stated that he had then decided that the crew should review the NNC “to ensure there were no actions he felt should be done or any other information they should be aware of." With the cabin altitude at 3,000 feet, he stated that “the crew felt safe to continue the flight” and four minutes after the cabin altitude warning had activated, clearance to continue the climb was requested and received.
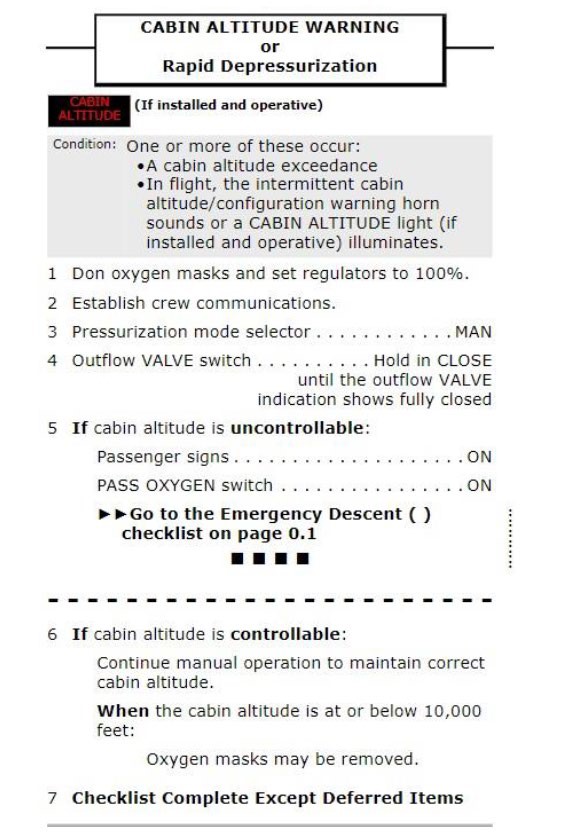
The Cabin Altitude Warning NNC. [Reproduced from the Official Report]
However, as FL200 was approached, a right air conditioning pack fault was annunciated and a second level-off there was requested and a corresponding clearance received. Actioning the applicable NNC did not restore normal function of the pack, and since the situation would impose limitations on the return sector, the captain contacted company Maintenance Control. It was agreed that the aircraft would return to Manchester. A 180° turn was made and descent from FL200 was commenced.
FDR data showed that the cabin altitude warning lights, which had illuminated on both pilot’s main panels when the aural warning began, had then remained on for 43 minutes. It was noted that these lights would be expected to automatically deactivate once between 500 feet and 1,500 feet below their 10,000 feet activation altitude. It was also noted that although it was not possible to recover data from the non-volatile memory (NVM) of the cabin pressurisation controllers, since the passenger cabin oxygen masks had not deployed, cabin altitude had not exceeded 14,000 feet.
The aircraft entered holding to burn off fuel and get below maximum landing weight. After 50 minutes in the hold, an approach and landing then followed after just over two hours airborne. No cause for the air conditioning pack fault was subsequently found but it was considered likely to have been a consequence of the air conditioning system being placed under a high load as a result of the crew selecting low temperatures.
Why It Happened
Overnight maintenance activity in connection with a recurrent right air conditioning pack fault had cleared the fault. However, the engineers involved had inadvertently failed to ensure that both engine bleed switches on the flight deck overhead panel had been returned to the normal ‘ON’ position. The aircraft had then been released to service without the line engineer overseeing the departure noticing the incorrect switch positions. The flight crew preflight check did not detect this either. The flight crew then failed to perform the After Takeoff check properly and because of that again failed to detect that both bleed switches were not in the correct position. This meant that as well as the cabin not pressurising, airframe and engine thermal anti-icing would not have been available and pressurisation of both the hydraulic reservoirs and the potable water tank would not have occurred. Also, with the engine bleeds off, an engine restart in flight would not have been possible.
When the cabin pressurisation warning was subsequently activated, the flight crew then failed to action the corresponding NNC for that warning. This resulted in the aircraft being operated by a flight crew at risk of hypoxia for a significant period of time, although with no sign of any consequences despite the extended time above 10,000 feet cabin altitude. It was accepted that “the likelihood of loss of consciousness is very small” but that nevertheless, such exposure would have the potential to “affect cognitive performance and decision making to the point where the decline would be observable in cognitive tests.” However, the reported added that below 14,000 feet it would be difficult to separate the relative contribution of hypoxia and other causes of suboptimal performance.
It was also noted that with the loss of an air conditioning pack, continued climb would have meant the aircraft would have pressurised at a rate of climb below that of the aircraft itself. This could have created a risk of progressive hypoxia that, if coupled with fatigue, “could have reduced the crew’s ability to respond appropriately to these indications."
Finally, it was noted that “in adverse weather where de-icing is required or if performance limitations require a no engine bleed takeoff, then the engine bleed switches may require manipulation before and after takeoff." However, whilst there were corresponding standard operating procedures (SOPs) for such circumstances, neither of them were applicable to the investigated flight issues.
The formal narrative Conclusion of the Investigation was recorded as follows:
The aircraft departed with the engine bleed air system off because the switches had been incorrectly left off following maintenance activity and had not been turned on during pre-flight procedures. The after-takeoff checklist is designed to trap the latter omission, but the incorrect switch selection went undetected by the crew. The aircraft failed to pressurise, but the crew did not complete the prescribed quick-reference handbook (QRH) drills in response to a cabin altitude warning, which remained illuminated for 43 minutes.
The Final Report was published on 5 December 2024. No safety recommendations were made.